

Breech Pregnancy and Birth
By Brandi Wood, DEM, CPM, CCE, CD
Breech presentation is an absolutely normal variation of pregnancy. Since the baby is in longitudinal lie, he can be born spontaneously.
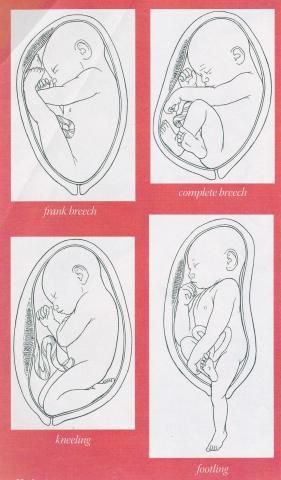
Four Major Types of Breech:
- Frank breech: the baby’s legs are extended and touch the head, occurs in about 65% of breech births.
- Complete breech: both knees are flexed and the feet tucked in beside the buttocks.
- Footling breech: neither hips nor knees are fully flexed. The feet are lower than the buttocks. This is very rare.
- Knee presentation: one or both hips are extended, with the knees flexed. This is also very rare.
Facts about breech presentation and birth:
- Breech presentation at term occurs in about three to four percent of all pregnancies.
- In births prior to 28 weeks the incidence of breech is about 25% (one-fourth of all breech babies are born = or < 30 weeks gestation).
- As pregnancy advances the baby moves to the head down position by the 34th week.
- Ninety-three percent of breech babies are born with no congenital abnormalities.
- Less than ten percent of women whose first baby was a breech presentation go on to have a second breech baby.
- Truly diabetic moms are three times more likely to have a breech baby.
- Maternal smoking during pregnancy is associated with a 30% higher risk of breech birth.
- Fetal anomalies are twice as frequent with breech babies as with those presenting head down.
- One in 50 babies who are breech at term are found to have neurological issues.
- One in 500 babies who are born in the breech position will die regardless of the method of birth.
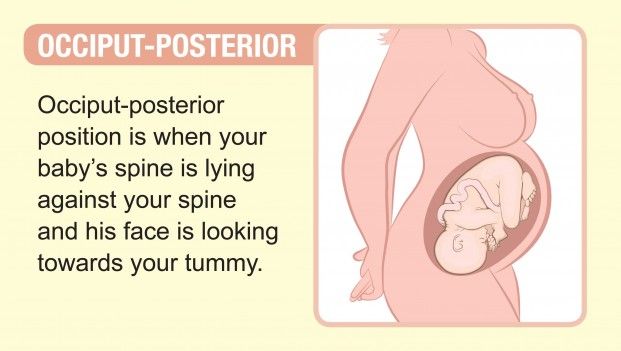
Occiput posterior: This position is similar to occiput anterior (the normal position), except that the baby faces the mother’s front, instead of her back. About 1 in 50 babies are positioned this way.
![]()
By Amanda Knowles
Transverse: A baby in the transverse position is sideways, usually with his shoulders or back over the cervix. Sometimes referred to as a shoulder or oblique position, a transverse position occurs in 1 in 2,500 births. The risk for having a baby in the transverse position increases if you go into labor prematurely, have given birth four or more times, or have placenta previa.
Types of breech birth

A) Complete, baby sits cross legged.
B) Incomplete is when one of the baby’s knees is bent and his foot and bottom are closest to the birth canal.
C) Frank breech, bottom first, legs up around the ears. this is the most common type of breech presentation.
D) Footling, either foot or feet coming first. This is the most common breech presentation for premature babies.
What causes breech presentation?
- Extended legs: the baby can’t turn head down because his/her legs are extended.
- Prematurity: since babies turn head down usually after the 34th week of pregnancy, breech presentation is common when preterm labor occurs.
- Twins, multiple pregnancy limits the space available for each baby to turn and can result in one or more babies presenting breech.
- Polyhydramnios: the mother has more amniotic fluid than average which, causes distention of the womb that can result in a breech presentation.
- Oligohydramnios: too little amniotic fluid so, the baby doesn’t have enough space to turn head down.
- Hydrocephaly (also known as hydrocephalus): the size of the baby’s head is increased because there is water on the brain and it might be more comfortable for him/her to be head up.
- Uterine abnormalities: any distortion of the cavity of the womb (e.g. fibroid tumors or a deviated septum) may result breech presentation.
- Cord entanglements/or short cord: around the baby’s neck or body.
- Amniotic bands: the amnion ruptures and some parts of the baby can entangle in the rolls which result in decreased freedom of movement.
- Tense, tight uterine and abdominal walls/or poor abdominal or uterine muscle tone: which prevent the baby from turning.
Risks of vaginal breech delivery: Breech births are riskier than the birth of a head down baby. Just how risky depends on the presentation, the reason for the presentation and maternal factors.
Possible risks and complications of breech vaginal delivery:
- Longer labors are associated with term breech babies as the weight and pressure of a head does not help dilate the cervix.
- If full cervical dilation is not reached there is a possibility of head entrapment.
- In a fast delivery, the head doesn’t have the opportunity to mold (as it does in head down presentation). This might result in bleeding within the baby’s skull.
- Cord prolapse: when the cord presents prior to the baby. This can occur because the buttocks, legs or knees don’t fit as tightly against the body. Cord prolapse is more common during premature birth. It is important to keep the membranes intact because they help cushion the cord. If cord prolapse happens early in labor, a cesarean section (C-section) will be recommended. If it occurs during the second stage, the birth may be continued but with an urgency. This complication is seen in 3.7 to 7% of breech babies and in approximately 0.3 percent of head down babies.
- The cord may become pinched between the head and the navel when the baby is born to the navel. However, cord compression is inevitable as the head passes through the pelvis.
- All of the above can lead to an increased need for suctioning of a breech baby and for neonatal resuscitation caused by asphyxia.
- Normal swelling and bruising of a baby’s presenting parts during labor and delivery.
- Injuries to internal organs: this is often caused by severe manipulation or incorrect handling of the breech birth. The most common injuries are liver, kidney or adrenal gland damage from pressure on the torso; neck or spinal injuries; and dislocated arms or legs; or fractures of the humerus, clavicle, skull and femur.
- It is possible for the placenta to separate when the baby’s head is still not born. This is called placental abruption.
- Fetal hypoxia: the baby doesn’t get enough oxygen. This may be due to cord prolapse, cord compression or premature separation of the placenta.
- Shoulder dystocia: extended arms over the head and behind the neck may result difficulty delivering the arms and shoulders.
- Increased fetal morbidity and mortality (injury and death): baby is more likely to die during breech birth because of the reasons stated above. Mortality is highest for the double footling presentation. Risks of serious early perinatal morbidity and mortality are three times higher for planned vaginal breech delivery than for an elective caesarean section.
Risks of cesarean section and benefits of vaginal birth:
- Cesarean section is major abdominal surgery.
- Picking up older children is discouraged for weeks or months after a cesarean section to allow proper healing after major abdominal surgery.
- Continuous support is needed both for your recovery and care of children and the house, to allow proper healing after major abdominal surgery.
- Risk of short term infection
- Higher risk of maternal death
- The scar on the uterus may complicate later pregnancies; it may decrease fertility; it can cause future miscarriages; ectopic pregnancies; premature separation of the placenta (placenta abruptio); or abnormally adherent placenta which may grow into the wall of the womb (placenta accreta); or placenta attached to lower segments of the womb (placenta previa).
- The risk of maternal death is 2.84 times greater after an elective cesarean section with no emergency present than if the mother had a vaginal birth
- There is the risk of morbidity with any abdominal surgery. These come from anesthetic accidents, damage to blood vessels during the procedure, an accidental extension of the uterine incision, or damage to internal organs, etc.
- Hemorrhage, anemia, infections and thrombosis are more common with a cesarean section than with a vaginal birth.
- There is a six percent chance for a breech baby to be accidentally cut by the surgeon during the cesarean procedure.
- Cesarean section is a potential risk factor for respiratory distress in infants.
- Prematurity is a related risk factor because elective cesareans are scheduled for the 38th week of pregnancy but the calculation of the time is often false. (When cesarean section is necessary or chosen, it should be performed after labor starts on its own.)
- There is a three to thirteen times increase in maternal mortality with cesarean section versus vaginal delivery when emergency and elective sections are included.
- Caesarean section is three times riskier than a vaginal birth. Higher maternal mortality and morbidity.
- Longer hospital stays.
- Greater risk of infection.
- Incidental and consequential morbidity from cesarean surgeries.
- Impact on future reproduction.
- Cesarean section is associated with higher fetal/ newborn morbidity, respiratory problems, bonding/ feeding problems, prematurity, etc. There is unequivocal data showing increased risk to the baby from cesarean section.
- Repeat caesarean sections: risks to the mother include: death, stroke, heart attack, pulmonary embolism, hemorrhage, infection, prolonged pain, hysterectomy, hospital readmission, adhesions (internal scar tissue), and infertility. And higher stillbirth, placenta previa, placental abruption rates in subsequent pregnancies.
- The risks increase with each caesarean section a woman has whereas the risk of uterine rupture decreases with each VBAC. (Mercer 2008)
- “The use of cesarean section for breech delivery in the belief that it is safer may become a self-fulfilling prophecy, as attendants become less skilled at breech delivery.” (Etkin e.t. al., 2000)
Benefits of a Vaginal Birth:
- Vaginal birth improves the baby’s chances of survival since the process of birth stimulates hormonal reactions in the baby.
- During vaginal birth you are actively involved in the birth process.
- Less risk of maternal morbidity and mortality.
- In well-chosen women there is no greater risk to baby versus caesarean.
- Increase in a woman’s right to choose.
- Reduces unnecessary caesarean sections.
- Prevents subsequent caesarean sections.
- Decreases likelihood of placenta acreta, and percreta due to previous cesarean.
- Because morbidity and mortality are relatively low, a large number of caesarean sections need to be performed to avoid a single adverse event.
You are the only one who can make the decision of whether to have a vaginal birth or elective cesarean and whether to birth at home or hospital. If you chose a vaginal birth, it is essential to have a practitioner experienced with breech deliveries — whether at home or hospital.
Can a breech presentation be changed?
Yes, it can! Here you can find techniques self-help and some that are performed by an experienced health care provider:
- Visualization of the baby: try to imagine your baby head down during pregnancy.
- Emotional factors may influence the presentation of the baby. If you are too busy, you live in an unstable emotional environment or you are afraid of birth your baby is prone to turn breech. Try to slow down and solve your problems. Pay attention to your baby and pregnancy. Talk to your baby, visualize your baby and have your partner to pay attention to your child. Have him talk to the baby right above the pubic bone.
- Breech tilt: you can start doing breech tilt exercises if you know your baby is breech from 30 to 32 weeks. Use an ironing board or other long flat surface and put one end to the height of a couch seat. Pad the board with a blanket and lay on it head down for 15 to 20 minutes, six to eight times daily. Massage your belly gently with both of your hands, put one hand above the baby’s bottom and the other above his head, move the face forward and the bottom upward in a rotating motion.
- Put a headphone on your belly close to your pubic bone and play soft music.
- Spinning babies has lots of exercises online and on their Daily Essentials DVD.
- There are some other techniques that can be performed by an experienced midwife, chiropractor or doctor. These external versions involve risk factors, talk to your health care provider to make an informed decision on the use of these techniques.
- Chiropractic care can be helpful during pregnancy especially with a chiropractor familiar with the Webster technique.
- External Cephalic Version (ECV) can be attempted by a skilled care provider after 36 weeks of gestation.
What will you feel during pregnancy?
- You will probably feel a hard lump under your ribs that can contribute to the discomfort of pregnancy.
- You will feel lots of movement low in your pelvis.
- Closer to the end of the pregnancy you can feel a hard round mass at the fundus, which is your baby’s head.
Delivery of the baby:
- The membranes may rupture earlier than with a head down baby. Your midwife will check to verify that there is no cord prolapse.
- The water may be stained with meconium that is the baby’s first stool because his belly is compressed.
- You can labor in any position. You can use the tub, birth stool, your bed, anything that appeals to you. It is recommended you be in an upright position as much as possible because gravity helps baby to be seated on the cervix.
- Eat and drink regularly and pee hourly during labor.
- When you feel an urge to push, your midwife will ask you not to push until she checks the cervix. It is very important that the cervix is fully dilated. You can feel the urge early and it may be hard not to push. Pay attention your midwife, she will help you and coach you through this difficult part.
- The midwife will wrap the baby in a warm blanket.
- The baby’s weight and the contractions will help the baby to be born to his/her shoulders. Then the baby will turn in order to deliver the shoulders. Then the body turns again and baby will be left to hang without support for one to two minutes. The baby’s weight will bring the head down. When the hairline appears, the midwife will grasp the baby’s ankle and lift the baby up until the nose and mouth are born. Then the midwife will most likely suction the mouth and nose.
- It seems to be common for breech babies to be slower to breath after being born. Be prepared that your baby may need some form of resuscitation. It occurs in about ten percent of cases.
- Visualize your baby during your pregnancy with the cord floating high in the womb, arms at his sides, his chin tucked to the chest, being born easily with very little blood loss, being pink, breathing right away after delivery and nursing well. Imagine your baby head down, in rare cases he may even turn during labor!
Term breech babies present their parents with a challenging decision:
- Should we go to the hospital and have a cesarean birth or should we attempt a vaginal breech birth at home?
- Breech birth in a hospital setting: In Central Indiana the majority of breech birth that happens in hospitals is via C-section.
- Breech birth in a home setting:
- Ensure your providers are trained in vaginal breech birth.
- Breech birth at home may proceed like any birth at home vaginally and un-medicated with especially close monitoring of mom and baby. Communication between the parents and midwife is crucial especially when the mom feels like pushing.
- In addition, another midwife will be called to attend the birth for an extra set of hands.
Home4Birth Requirements for Considering a Vaginal Breech Birth at Home:
- A well informed woman and partner who are both, after learning the risks and benefits and considering their options, very committed to birth at home.
- An ultrasound to determine position of the baby’s feet.
- At least three sets of hands present and preferably one of them being another midwife.
- Receiving good informed consent and a signing this form.
- Chiropractic visits that utilize the Webster technique to encourage the baby to turn.
- Use of spinning babies techniques to encourage the baby to turn to a vertex presentation.
- Parents consider an external cephalic version which is a procedure that can halve the number of breech presentations but the procedure is not risk-free.
Other Resources for Information and Research on Breech Birth Safety/ Suggested Reading:
Maggie Banks: Breech Birth, Woman-Wise (available for checkout in Home4Birth’s library)
Benna Waites: Breech Birth (available for checkout in Home4Birth’s library)
Heads Up! All about Breech Babies (turning techniques, studies, videos for sale, stories, & articles)
ICAN (International Cesarean Awareness Network)
Incredible detailed pictures of a great natural breech birth (hospital born)
Resources:
- Baldwin: Special Delivery (available for checkout in Home4Birth’s library)
- Anne Frye: Holistic Midwifery, Vol. I. (available for checkout in Home4Birth’s library)
- Langer; E. Boudier; G. Schlaeder: Breech Presentation after 34 Weeks-a Meta-Analysis of Corrected Perinatal Mortality/Morbidity According to the Method of Delivery
- Myles: Textbook for Midwives (available for checkout in Home4Birth’s library)
- Enkin e.t. al.: A Guide to Effective Care in Pregnancy and Childbirth
- Waites, Benna: Breech Birth, 2003 (available for checkout in Home4Birth’s library)
- Chopra S e.t. al.: Disengagement of the Deeply Engaged Fetal Head during Cesarean Section in Advanced Labor: Conventional Method Versus Reverse Breech Extraction, https://www.ncbi.nlm.nih.gov/pubmed/19925377, Acta Obstetricia et Gynecologica Scandinavica. 88.10 (Oct 2009): 1163–1166
- Kolas e.t. al.: Planned Cesarean Versus Planned Vaginal Delivery at Term: Comparison of Newborn Infant Outcomes, https://www.ncbi.nlm.nih.gov/pubmed/16846577, American Journal of Obstetrics & Gynecology (2006) 195, 1538–43.
- Rageth e.t. al.: Delivery after Previous Cesarean: a Risk Evaluation. Obstetrics & Gynecology, https://journals.lww.com/greenjournal/Abstract/1999/03000/Delivery_After_Previous_Cesarean__A_Risk.3.aspx#:~:text=The%20risk%20of%20uterine%20rupture,%2C%200.56)%2C%20were%20lower., 93.3 (March 1999): 332-337
- Alarah, M., Regan, C., O’Connell, M.P., Keane, D.P., O’Herlihy, C., & Foley, M.E.: Singleton Vaginal Breech Delivery at Term: Still a Safe Option. The American Congress of Obstetricians and Gynecologists (ACOG) (2004), 103(3), 407-412
- Banks, M.: Active Breech Birth: The Point Of Least Resistance, New Zealand College of Midwives Journal, (2007), 36, 6
- Banks, M.: Breech Birth Beyond the “Term Breech Trial” www.Birthspirit.Co.Nz, (2001) Retrieved July 22, 2011
- Banks, M.: Term Breech New Zealand College of Midwives Midwifery News, (2000), (20), 25-26.
- Daviss, B.A., Johnson, K.C. & Lalonde, A.B.: Evolving Evidence since the Term Breech Trial: Canadian Response, European Dissent, and Potential Solutions. (2010) Journal of Obstetrics and Gynaecology Canada (JOGC), 217-224
- Giuliani, A. e.t. al.: Mode of Delivery and Outcome of 699 Singleton Breech Deliveries at a Single Center. American Journal of Obstetrics & Gynecology, (2002) 187, 1694-1698
- Hannah, M.E., Hannah, W.J., Hewson, S.A., Hodnett, E.D., Saigal, S. and Willan, A.R.: Planned Caesarean Section versus Planned Vaginal Birth for Breech Presentation at Term: a Randomized Multicentre Trial. The Lancet, (2000) 356, 1375-1383, https://www.ncbi.nlm.nih.gov/pubmed/11052579, Retrieved July 22, 2011
- Keirse, M.J.N.C.: Evidence-Based Childbirth Only For Breech Babies? Birth, (2004), 29(1), 55-59
- Kotaska, A.: Breech Birth Can Be Safe, But is it Worth the Effort? JOGC, (2009), 31(6), 553-554
- LaLonde, A.B.: Vaginal Breech Delivery Guideline: the Time Has Come. JOGC, (2009), 31(6), 483-484
- SOGC Clinical Practice Guideline: Vaginal Delivery of Breech JOGC, (2009), (226), 557-566
- Goer, Henci: The Thinking Woman’s Guide to a Better Birth. Section 2. 1999: Perigee Books
- Breech Babies: What Can I Do If My Baby Is Breech? American Academy of Family Physicians Riverside Midwifery, LLC. https://familydoctor.org/breech-babies-what-can-i-do-if-my-baby-is-breech/
- What Should I Know About Cesarean Section?, Childbirth Connection
- Patient Choice Vaginal Delivery? Annals of Family Medicine: http://www.annfammed.org/content/4/3/265.abstract
- If Your Baby Is Breech: American College of Obstetricians and Gynecologists, http://www.drshanbourmd.com/webdocuments/ACOG-If-Your-Baby-Breech.pdf
- Five Years to the Term Breech Trial: the Rise and Fall of a Randomized Controlled Trial, (2006-01) https://pubmed.ncbi.nlm.nih.gov/16389006/
- Is Planned Vaginal Delivery for Breech Presentation at Term Still an Option? Results of an Observational Prospective Survey in France and Belgium, (2006-02) https://pubmed.ncbi.nlm.nih.gov/16580289/#:~:text=Conclusion%3A%20In%20places%20where%20planned,can%20be%20offered%20to%20women.
- ACOG Committee Opinion No. 340. Mode of Term Singleton Breech Delivery, (2006-03) https://pubmed.ncbi.nlm.nih.gov/16816088/
- The Effect of the Term Breech Trial on Medical Intervention Behaviour and Neonatal Outcome in the Netherlands: an Analysis of 35,453 Term Breech Infants, (2005-01) https://obgyn.onlinelibrary.wiley.com/doi/abs/10.1111/j.1471-0528.2004.00317.x
- Term Breech Delivery in Sweden: Mortality Relative to Fetal Presentation and Planned Mode of Delivery, (2005-02) https://obgyn.onlinelibrary.wiley.com/doi/pdf/10.1111/j.0001-6349.2005.00852.x#:~:text=Results.,2.7%2C%202.1%E2%80%933.6).
- Outcomes of Children at 2 Years After Planned Cesarean Birth Versus Planned Vaginal Birth for Breech Presentation at Term: the International Randomized Term Breech Trial, (2004-01) https://pubmed.ncbi.nlm.nih.gov/15467555/
- Planned Caesarean Section for Term Breech Delivery, https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000166/full (2003-01)